

Carpal Tunnel Syndrome
 Carpal tunnel syndrome (known as CTS) is an entrapment syndrome that develops from an increase in pressure on the median nerve at the wrist. The increased pressure begins to pinch the nerve and often results in tingling, numbness and pain felt in the fingers, hand, wrist and arm. The carpal tunnel is a space where the median nerve, along with nine tendons, cross from the forearm, through the wrist and into the hand. If the pressure gets too high and starts interfering with the nerve’s function, quickly the CTS symptoms mentioned above can result. Many people feel CTS symptoms at night and predominantly in the middle finger, index finger and thumb. Loss of strength in the hand, trouble coordinating the fingers and performing acts of daily living (holding a tooth brush, reading the newspaper, driving) could all be signs of CTS. It is highly recommended you make an appointment to see an experienced hand surgeon if you are experiencing any of the symptoms of carpal tunnel syndrome.
Carpal tunnel syndrome (known as CTS) is an entrapment syndrome that develops from an increase in pressure on the median nerve at the wrist. The increased pressure begins to pinch the nerve and often results in tingling, numbness and pain felt in the fingers, hand, wrist and arm. The carpal tunnel is a space where the median nerve, along with nine tendons, cross from the forearm, through the wrist and into the hand. If the pressure gets too high and starts interfering with the nerve’s function, quickly the CTS symptoms mentioned above can result. Many people feel CTS symptoms at night and predominantly in the middle finger, index finger and thumb. Loss of strength in the hand, trouble coordinating the fingers and performing acts of daily living (holding a tooth brush, reading the newspaper, driving) could all be signs of CTS. It is highly recommended you make an appointment to see an experienced hand surgeon if you are experiencing any of the symptoms of carpal tunnel syndrome.
If treated in time, CTS can be treated without surgery with a splint and a steroid injection. However, if pain does not subside with noninvasive treatment, some cases will require surgery to relieve pressure on the median nerve.
Dr.Lucchina prefers, if possible, to perform noninvasive surgery to open the carpal tunnel, i.e to make an endoscopic or US-guided carpal tunnel release, with a faster recovery-time in the first 3 months and a better scar appearance.
The surgical procedure is usually less than 15 minutes long, performed as outpatient with a local anesthesia and absorbable sutures.
During the procedure by the use of small cameras, knives and scissors the skin is cut (superficial incisions 1,5 cm long) and the carpal tunnel is incised longitudinally and left open. From the first night postsurgery on our patients experience a sudden improvement (or complete disappearance) from previous pain, tingling and numbness of the fingertips and restart sleeping. The use of absorbable sutures and really active local anesthetics and oral pain killers renders the procedure almost pain-free. Postsurgery no splints are worn, and a complete active range of motion of fingers and wrist and an immediate recovery for activities of daily living or sports activities is allowed. The use of heavy tools is allowed after 3/4 weeks.
Cubital Tunnel Syndrome
 Cubital tunnel syndrome is the result of an increased pressure on the ulnar nerve at the elbow. The ulnar nerve passes alongside the bone on the medial epicondyle and is very vulnerable to increased pressure. If the increase in pressure is too great on the ulnar nerve, it can cause numbness, tingling and pain in the elbow, lower arm, wrist, hand and fingers. Cubital tunnel syndrome is caused by a variety of things, including prolonged elbow bending (like reading a magazine or answering to the telephone), resting the inner part of the elbow on a table or chair or the nerve being shifted around against the medial condyle too much to the point where irritation of the ulnar nerve results.
Cubital tunnel syndrome is the result of an increased pressure on the ulnar nerve at the elbow. The ulnar nerve passes alongside the bone on the medial epicondyle and is very vulnerable to increased pressure. If the increase in pressure is too great on the ulnar nerve, it can cause numbness, tingling and pain in the elbow, lower arm, wrist, hand and fingers. Cubital tunnel syndrome is caused by a variety of things, including prolonged elbow bending (like reading a magazine or answering to the telephone), resting the inner part of the elbow on a table or chair or the nerve being shifted around against the medial condyle too much to the point where irritation of the ulnar nerve results.
Treatment is usually non-invasive, but in some instances, surgery is needed to relieve the pain. The most common surgeries include repositioning the ulnar nerve onto the front of the elbow or sometimes the medial epicondyle will be altered to better accommodate the nerve.
Dr.Lucchina prefers, if possible, to perform mini-invasive surgery to open the cubital tunnel, i.e to make an endoscopic cubital tunnel release, with a faster recovery-time and a better scar appearance.
The operative procedure is usually less than 45 minutes long, performed as outpatient with a local anesthesia and absorbable sutures.
During the procedure by the use of small cameras, knives and scissors the skin is cut (superficial incisions 3 cm long) and the cubital tunnel at the elbow is incised longitudinally and left open. From the first night postoperatively on our patients experience a sudden improvement from previous pain, tingling and numbness of the fingertips and restart sleeping. The use of absorbable sutures and really active local anesthetics and oral pain killers renders the procedure almost pain-free. Postoperatively no splints are worn but a hyperflexion of the elbow for the first 4 weeks is not recommended. A complete active range of motion of fingers and wrist and an immediate recovery for activities of daily living or sports activities is strongly recommended. The use of heavy tools is allowed after 3/4 weeks.
De Quervain’s tenosynovitis
 De Quervain’s tenosynovitis is an inflammation of the tendons on the side of the thumb which can be very painful. Common symptoms of De Quervain’s tenosynovitis usually include an aching pain in the thumb every time it is moved, including turning the wrist, making a fist or trying to grasp something.
De Quervain’s tenosynovitis is an inflammation of the tendons on the side of the thumb which can be very painful. Common symptoms of De Quervain’s tenosynovitis usually include an aching pain in the thumb every time it is moved, including turning the wrist, making a fist or trying to grasp something.
While the definitive cause of De Quervain’s tenosynovitis is not known, any repetitive motion of the hand or wrist is thought to worsen the condition, including playing music, typing, playing video games, excessive smart phone usage and cooking—just to name a few.
Treatment usually consists of identifying and altering repetitive motions that are causing the pain, immobilizing the wrist, medication, steroid injection, TECAR-therapy and in severe cases, surgery. You will want to consult with an experienced hand surgeon first to make sure operating is the best option after a failure of all conservative treatments. Surgical operation consists of extensor tendon tenolysis.
The operative procedure is usually less than 20 minutes long, performed as outpatient with a local anesthesia and absorbable sutures.
During the procedure by the use of small instruments the skin is cut (superficial incision 2 cm long) and the tendon sheath at the wrist is incised longitudinally and left open. From the first night postoperatively on our patients experience a sudden improvement from previous pain and tendons blockade and restart sleeping. The use of absorbable sutures and really active local anesthetics and oral pain killers renders the procedure almost pain-free. Postoperatively a splint to protect the scar is worn for 1 week but the thumb fingertip is left free so a complete active range of motion of fingers and wrist and an immediate recovery for activities of daily living or sports activities is strongly recommended. The use of heavy tools is allowed after 3/4 weeks
Dupuytren’s Disease
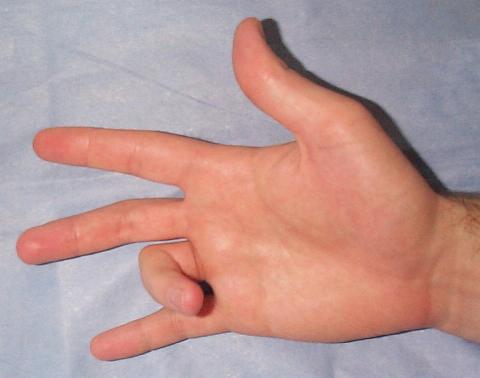
 Dupuytren’s disease also known as Dupuytren’s Contracture or “Viking’s Disease” is a condition where the hand becomes deformed with a typical finger flexion. Dupuytren’s Disease is a progressive hardening, shortening and knotting of connective tissue in the palm. This results in a permanent bending of the fingers (usually the little and ring finger). The condition is usually painless, but some people experience discomfort as the connective tissue becomes less flexible.
Dupuytren’s disease also known as Dupuytren’s Contracture or “Viking’s Disease” is a condition where the hand becomes deformed with a typical finger flexion. Dupuytren’s Disease is a progressive hardening, shortening and knotting of connective tissue in the palm. This results in a permanent bending of the fingers (usually the little and ring finger). The condition is usually painless, but some people experience discomfort as the connective tissue becomes less flexible.
Because the hand cannot be flattened or the fingers completely straightened, acts of daily living are adversely affected. Dupuytren’s disease usually occurs in older males, but can be found in women as well.
Treatments include stretching and splinting in the early stages, but more advanced cases may require surgical treatment to help straighten the fingers and release the tissue buildup in the palm. In recent years the collagenase injection or a office-based percutaneous cordotomy are useful ways to cure this pathology in early stages.
In the last years a liposuction from the abdominal wall with a fat graft transplantation to the hand has improved the aesthetics of the scar and the function of the hand as a whole in the immediate post-operative period.
Fracture of the hand and Mini invasive Tools
 Dr.Lucchina and his support team specialize in complex hand and wrist fractures including distal radius fractures. The hand and wrist contain many bones and joints and early consulting with an experienced hand and wrist surgeon is crucial to proper treatment and an optimal healing.
Dr.Lucchina and his support team specialize in complex hand and wrist fractures including distal radius fractures. The hand and wrist contain many bones and joints and early consulting with an experienced hand and wrist surgeon is crucial to proper treatment and an optimal healing.
Dr.Lucchina has extensive experience in treating and operating on severe crushing and traumatic hand, wrist and forearm injuries, resulting from machine, sports, automobile and boating accidents including distal radius fractures, metacarpal and phalangeal fractures.
The operative procedures are usually less than 1 hour long, performed as outpatient with a local anesthesia and absorbable sutures.
During the procedure by the use of small instruments the skin is cut, the fracture is reduced with special maneuvers and then fixed with stable adn mini-invasive tools. From the first night postoperatively on our patients experience a sudden improvement from previous pain due to the anatomical bone recontruction. The use of absorbable sutures and really active local anesthetics and oral pain killers renders the procedure well-accepted and recommended. Postoperatively a splint to protect the scar and the fracture is worn for about 1 week.
The use of advanced technical devices and particular plate, screws and braces allow an immediate active range of motion the day after the operation, with early recovery for activities of daily living in 3/4 weeks and manual works in 3/6 weeks.
Scaphoid fractures
They represent the most frequent fracture of the carpal bones (about 85%), are often unrecognized at the first visit so the correct treatment is frequently delayed as well as the bone healing. The scaphoid is the “pivot-bone” inside the wrist joint that allows a painless and normal active movement of the wrist. It’s usually divided into three parts from distal to proximal, i.e. the tubercle, the waist and the proximal pole.
The vascularization of this small bone comes from the distal part (the tubercle) and is directed towards the proximal part (proximal pole). Due to the reduced vascularization of this carpal bone, the main complication associated with scaphoid fractures is “non-union” (no bone healing) or avascular necrosis of the proximal pole, that is the closest part to the wrist joint.
A delayed diagnosis with a non-union or necrosis of the scaphoid leads to a secondary joint arthritis with severe impairment for activities of daily living. In these not rare cases, only a surgical procedure can reduce pain and functional limitations restoring a nearly normal wrist anatomy.
In addition to traditional clinical and radiographic examination really useful are CT and MRI done at early stages, the latter in particular to study the vascularization of the fractured bony portion, closest to the wrist. The type of bone fracture, the age and job of the patient are the main factors determining the final best therapeutic choice.
For dislocated fractures and fractures of the proximal part, bone fixation with a headless screws is mandatory. The last generation screws can provide a mechanical stability with a reduced healing time compared to the cast immobilization which is about 8-12 weeks and really high consolidation rate. Usually for the bone to be fixed an open approach with incisions 3-4 cm long at the wrist is used. The operation, performed in local anesthesia and as outpatient, is about 60 minutes long.
More recently for not dislocated fractures, a percutaneous fixation with a screw is possible. In these cases a 1-cm incision on the volar side of the wrist is used and the screw is inserted with a particular technique and special devices with a good cosmetic result and reduced post-operative pain. For particular patients requiring an immediate range of motion or that cannot wear casts this technique is particularly indicated and appreciated.
Ganglion Cysts
 Ganglion cysts are lumps that form in the hand and wrist and sometimes in the foot as well. They are non-cancerous fluid-filled sacs that usually occur along joints or tendons.
Ganglion cysts are lumps that form in the hand and wrist and sometimes in the foot as well. They are non-cancerous fluid-filled sacs that usually occur along joints or tendons.
The cause of ganglion cysts is unknown but can be secondary to a previous trauma. They can appear suddenly or slowly grow over time.
If you wish to remove a ganglion cyst due to impaired joint movement or discomfort, make sure to contact an experienced hand surgeon for a consultation to decide the best approach for treatment.
The operative procedure is usually less than 45 minutes long, performed as outpatient with a local anesthesia and absorbable sutures.
During the procedure by the use of small instruments the skin is cut dorsally (superficial incision 2 cm long) and the ganglion is excised. From the first night postoperatively on our patients experience a sudden improvement from previous pain. The use of absorbable sutures and really active local anesthetics and oral pain killers renders the procedure almost pain-free. Postoperatively a splint to protect the scar is worn for 1 week but the thumb and long fingers are left free so a complete active range of motion of fingers and wrist and an immediate recovery for activities of daily living or sports activities is strongly recommended. The use of heavy tools is allowed after 3/4 weeks
Trigger Finger
 Trigger finger, medically known as stenosing tenosynovitis, is when one of the fingers or thumbs momentarily gets stuck in a bent position and then painfully snaps when straightened back. In severe cases, the finger being affected can become locked in a flexed position requiring release by a hand doctor or surgeon.
Trigger finger, medically known as stenosing tenosynovitis, is when one of the fingers or thumbs momentarily gets stuck in a bent position and then painfully snaps when straightened back. In severe cases, the finger being affected can become locked in a flexed position requiring release by a hand doctor or surgeon.
Trigger finger is caused by the narrowing of the tendon sheath within the finger. Trigger finger is more prevalent in women, people with diabetes and those performing repetitive gripping movements for work or hobbies.
Treatment for trigger finger varies, depending on the severity. Conservative treatment usually includes splinting, hand exercises, the use of nonsteroidal anti-inflammatory drugs (NSAIDs) or a steroid injection. In more than 80% of cases one visit only is needed to solve the problem in 1-6 weeks. More severe cases may require a trigger finger release surgery.
Surgery consists of flexor tendon tenolysis with opening of the tendon sheath in the palm.
The surgical procedure is usually less than 15 minutes long, performed as outpatient with a local anesthesia and absorbable sutures.
During the procedure by the use of small instruments the skin is cut palmarly (superficial incision 2 cm long) and the sheath is longitudinally incised and left open. From the first night postsurgery, on our patients experience a sudden improvement from previous pain with a complete recvovery of the active finger range of motion. The use of absorbable sutures and really active local anesthetics and oral pain killers renders the procedure almost pain-free. Post surgery no splints are needed and both the thumb and long fingers are left free.
A complete active range of motion of fingers and wrist and an immediate recovery for activities of daily living or sports activities is strongly recommended. The use of heavy tools is allowed after 3/4 weeks
WRIST AND SMALL JOINTS ARTHROSCOPY
 Arthoscopy is a minimally invasive surgical technique developed over three decades ago in order to explore a joint from within. Tiny incisions are used to insert a camera to the inside of a joint and allows a surgeon to not only diagnose a problem but often times allows definitive treatment. This is opposed to the more standard technique of open joint surgery, which can result in increased painful scarring and prolonged recovery time. More recently, general and gynecologic surgery have also benefited from these endoscopic techniques and joint arthroscopy surgery has enjoyed great success in orthopaedic surgery (knee, shoulder, hip). Smaller joints now have also benefited from this technique. A smaller arthroscope (2.7 or even 1.9 mm) has been devised in order to diagnose and even treat wrist pathology, which up until now has been a problem area. We have even used arthroscopic techniques to treat pathology in the basal joint of the thumb and knuckle joint of the
Arthoscopy is a minimally invasive surgical technique developed over three decades ago in order to explore a joint from within. Tiny incisions are used to insert a camera to the inside of a joint and allows a surgeon to not only diagnose a problem but often times allows definitive treatment. This is opposed to the more standard technique of open joint surgery, which can result in increased painful scarring and prolonged recovery time. More recently, general and gynecologic surgery have also benefited from these endoscopic techniques and joint arthroscopy surgery has enjoyed great success in orthopaedic surgery (knee, shoulder, hip). Smaller joints now have also benefited from this technique. A smaller arthroscope (2.7 or even 1.9 mm) has been devised in order to diagnose and even treat wrist pathology, which up until now has been a problem area. We have even used arthroscopic techniques to treat pathology in the basal joint of the thumb and knuckle joint of the
hand.The wrist is widely regarded as the most complex joint in the human body. There are eight carpal bones, which articulate with the two forearm bones creating a joint that moves in multiple planes. Wrist pain until recently, has often eluded doctors due to the complexity and small size of this joint. Even MRI technology still cannot elucidate subtle problems with this articulation. The carpal bones are held together by small ligaments, which are often the subject of trauma and can lead to instability of these bones, leading to posttraumatic arthritis in the future.The triangular fibrocartilage is a small cartilage disc, similar to the meniscus in the knee, which often leads to wrist pain along the ulnar side of the wrist and irradiated to the forearm. Tears in these ligaments can now be diagnosed and either debrided or repaired using arthoscopic means. The artroscope can also be used to resect inflamed joint tissue (synovium), remove bony, loose
bodies, or treat articular fracture. As in other joints arthroscopy has broadened the horizons in hand and wrist arthroscopy surgery leading to improved diagnosis and treatment of complex problems that were untreatable in the past or underdiagnosed.
The surgical procedure is usually less than 45 minutes long, performed as outpatient with a local anesthesia and absorbable sutures.
During the procedure by the use of small cameras, probes, knives and scissors the skin is cut (superficial incisions 1 cm long) and the wrist is inspected and any intraarticular lesion is addressed. The use of absorbable sutures and really active local anesthetics and oral pain killers renders the procedure almost pain-free.
Postsurgery, a splint for at least 1 week is worn then a physiotherapic protocol is promptly started depending on the surgical procedure performed. A complete active range of motion of fingers and wrist and an immediate recovery for activities of daily living or sports activities is strongly recommended. The use of heavy tools is allowed after 3/4 weeks.
BASAL THUMB JOINT ARTHRITIS
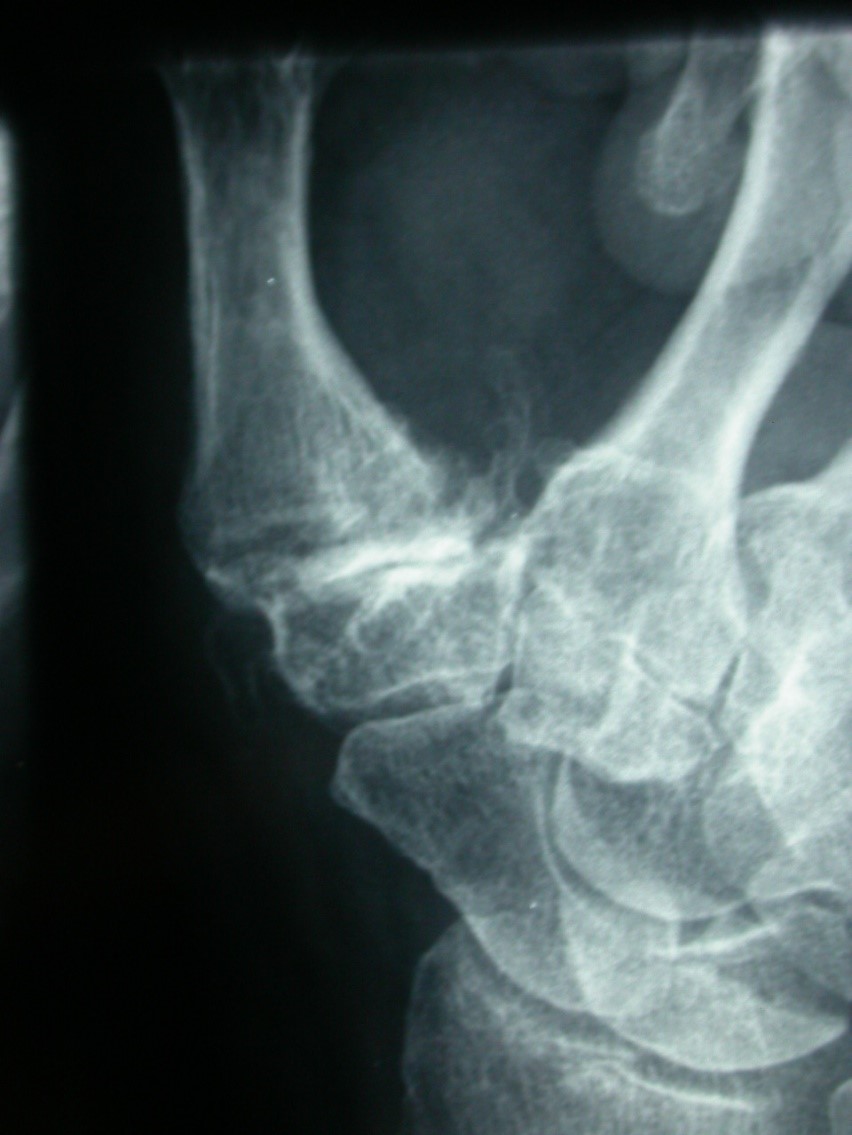 Thumb arthritis is the most common form of osteoarthritis affecting the hand. Also called basal joint arthritis, thumb arthritis occurs when the cushioning cartilage wears away from the adjoining ends of the bones that form your thumb joint (carpometacarpal joint). Thumb arthritis can cause severe hand pain, swelling, and decreased strength and range of motion, making it difficult to do simple household tasks, such as turning doorknobs and opening jars.
Thumb arthritis is the most common form of osteoarthritis affecting the hand. Also called basal joint arthritis, thumb arthritis occurs when the cushioning cartilage wears away from the adjoining ends of the bones that form your thumb joint (carpometacarpal joint). Thumb arthritis can cause severe hand pain, swelling, and decreased strength and range of motion, making it difficult to do simple household tasks, such as turning doorknobs and opening jars.
At the beginning pain starts while performing activities with thumb rotation. Treatment for thumb arthritis may include self-care measures, vitamins reducing cartilage loss, splints, non-steroidal anti-inflammatory drugs or eco-guided hyaluronic acid injections in the early stages. The use of high-molecular weight hyaluronic acid increases the visco-elasticity with a secondary increase of the joint mobility and less local pain.
In selected cases long lasting pain relief can be achieved by intra-articular corticosteroid injections or PRP (platelet-rich-plasma) containing growth factors. Moreover in the last months a liposuction from the abdominal wall with an arthroscopically assisted fat graft transplantation to the hand has improved the function of the hand as a whole in the immediate post-operative period.
The surgical procedure is usually 1 hour long, performed as outpatient with a local anesthesia and absorbable sutures.
During the procedure by the use of small instruments the skin is cut (2 superficial incision 3 cm long) and the trapezium bone is removed. From the first night postoperatively on our patients experience a sudden improvement from previous pain and functional limitations. The use of absorbable sutures and really active local anesthetics and oral pain killers renders the procedure almost pain-free. A postsurgery thumb splint with all the other fingers completely free is worn for 3 weeks then a complete active range of motion of fingers and wrist is allowed with an immediate recovery for activities of daily living or sports. The use of heavy tools is allowed after 6/8 weeks.
TENNIS ELBOW
 Tennis elbow, or lateral epicondylitis (LE), is a painful condition of the elbow caused by overuse. Not surprisingly, playing tennis or other racquet sports can cause this condition. But several other sports and activities can also put you at risk, in particular gardeners, wood cutters or workers in supermarkets.
Tennis elbow, or lateral epicondylitis (LE), is a painful condition of the elbow caused by overuse. Not surprisingly, playing tennis or other racquet sports can cause this condition. But several other sports and activities can also put you at risk, in particular gardeners, wood cutters or workers in supermarkets.
Tennis elbow is an inflammation of the tendons that join the forearm muscles on the outside of the elbow. The forearm muscles and tendons become damaged from overuse — repeating the same motions again and again. This leads to pain and tenderness on the outside of the elbow.
The condition causes pain on the outside portion of the elbow over a bony prominence named the lateral epicondyle. Pain occurs with activities such as grasping, pushing, pulling, and lifting. As the process progresses, the pain may occur with limited activities or even at rest. Of note, a separate entity termed golfers elbow, or medial epicondylitis, causes pain on the inside of the elbow.
Anatomy
The lateral epicondyle is where the Extensor Carpi Radialis Brevis (ECRB) and Extensor digitorum communis (EDC) tendon inserts. This tendons attaches to the muscle that allows your wrist and fingers to extend.
Diagnosis
The diagnosis is usually made based on the history that the patient describes to the healthcare provider, and a physical exam. There will be localized tenderness in the region of the lateral epicondyle. Pain is also often reproduced with the patient extending their wrist under resistance.
X-rays may be done to rule out other causes of elbow pain; however, these are typically normal. Other imaging modalities, such as US (ultrasound) and MRI (magnetic resonance imaging) con confirm the diagnose and show the presence of microcalcification addressing the most correct therapy
There are many treatment options for tennis elbow. In most cases, treatment involves a team approach. Primary doctors, physical therapists, and, in some cases, surgeons work together to provide the most effective care.
Treatment – Nonsurgical
Treatment Nonsurgical treatment mainly focuses on addressing the symptoms, but do not resolve the cause of the pain.
I’m used to tell my patients that the strategy to solve a lateral epicondylitis is like a pyramid. At the base there is the bottom floor. In the case of failure you’re bound to step over.
Rest and proper stretching is the first step, combined with anti-inflammatory medications and a palmar splint. Stretching is focused on the wrist extensor muscles. First, the extensor muscles are stretched with the elbow held in flexion, and later with the elbow extended. Finally, strengthening exercises are performed, focused on the extensor muscles. The use of splints, to reduce the extension against resistance of the wrist are a valid device to help the healing process or in addition to further treatments.
One step over stays a corticosteroid (CS) injection. Everybody knows pros and versus of their use. I don’t like CSs so much for the risk of secondary appearance of painful deposits that are worse than the initial clinical condition. But It represents the most used (and for someone the most effective) drug.
One step over stay the high-frequency shock waves. I think they’re really operator-dependant and effective in case of microcalcification due to a long-lasting problem.
One step over there is the use of TECARtherapy one of the most used and most effective therapy since 15 years ago for human tendinitis especially in sportsmen.
One step over stays an Aethoxysclerol injection. It’s a US-guided injection of a drug with proven anti-inflammatory effect in Achilles tendinitis and lateral epicondylitis.
One step over stays the PRP (platelet-rich-plasma) injection. A series of 3 injections are made in 1/2 weeks at the insertion site of the affected tendons. It’s one of the newest therapy used to deal with LE and with early extraodinary results. It’s based on the ability of a platelet derived growth factor to make tendon tears heal.
When all conservative therapies have failed, on top of the pyramid stays the surgeon. It happens one case out 20.
I’m used to perform a mini-invasive surgery, so-called tenolyse, removing all tendon tears and all areas of tenomalacia and restoring the normal anatomy with great improvement in all cases.
The surgical procedure procedure is usually 45 minutes long, performed as outpatient with a local anesthesia and absorbable sutures.
The surgical procedure is usually 45 minutes long, performed as outpatient with a local anesthesia and absorbable sutures.
During the procedure by the use of small instruments the skin is cut (incisions 3 cm long) and the tendon tears are removed at the lateral epicondyle. From the first night postoperatively on our patients experience a sudden improvement from previous pain and functional limitations. The use of absorbable sutures and really active local anesthetics and oral pain killers renders the procedure almost pain-free. A postsurgery splint for a few days is worn then a complete active range of motion of fingers, wrist and elbow is allowed with an immediate recovery for activities of daily living. The use of heavy tools is allowed after 6/8 weeks.
SURGERY FOR NEUROLOGIC PATIENTS
 Lots of patients affected by cerebrovascular accidents and traumatic brain injuries share many features. Lesions of the central nervous system, the peripheral nervous system and the muscoloskeletal system and lesions causing pain may lead directly or indirectly to syndromes of restricted or excessive motion of the limbs.
Lots of patients affected by cerebrovascular accidents and traumatic brain injuries share many features. Lesions of the central nervous system, the peripheral nervous system and the muscoloskeletal system and lesions causing pain may lead directly or indirectly to syndromes of restricted or excessive motion of the limbs.
Spasticity is a disorder of muscle function that causes muscle tightness or spasm. It is the involuntary movement (jerking) of muscles, which occurs when there is damage to the central nervous system. This damage may result from a traumatic brain injury, stroke, tumor, cerebral palsy or multiple sclerosis. Symptoms may include hypertonicity (increased muscle tone), clonus (a series of rapid muscle contractions), exaggerated deep tendon reflexes, muscle spasms, scissoring (involuntary crossing of the legs), and fixed joints. Spasticity may be as mild as the feeling of stiffness or tightness of muscles, or it may be so severe as to produce painful uncontrollable spasms of the extremities. It may also produce feelings of pain or tightness in and around joints. Some people find that spasticity is so severe or frequent that it disrupts their life. Health care professional suggest a number of things to calm or stop spasticity: range-of- motion exercises, stress management, prescription drugs, physical therapy regimens, and or surgery.One treatment method that has consistently produced positive results for spasticity patients is the injection of Botulinum toxin, or BOTOX. 
BOTOX is injected directly into the spastic muscle with the person receiving a dose according to body weight.It is has been my mentors and my experience that less importance has been given to the muscolo-skeletal impairment that results from brain trauma or stroke. For a surgeon is really sad to walk in the streets or to see patients admitted in the hospital for other reasons with enormous physical impairment at the upper extremity undertreated or with a potential large improvement from little surgery and NEVER REFERRED.
Surgery can play a very important role in the treatment of chronic spasticity and may achieve three goals: hygiene, cosmesis, function restore. Musculoskeletal surgery is the most frequently used surgical procedure for spasticity and is performed on the muscle or tendon itself. Tendon lengthening tenoplasty or tendon transfer, joint fusions, bone osteotomies are often effective and successful in reducing the tension on the muscle, thereby reducing tightness, spasticity and pain. A postsurgery splint for a few days is worn then a complete passive or active range of motion of fingers, wrist and elbow is allowed with an immediate recovery for activities of daily living depending on the pre-surgery status and limitations. The use of heavy tools is allowed after 4/6 weeks. Night splints to maintain the improvements are usually worn for 2/3 months.x